Discussion Group: March 2023
Introduction
We introduced ourselves and the story of the podcast, which you can again HERE. We also shared that we have written a memoir, a lived experience workbook, and a clinical compilation. Pictures of, information about, and links to those resources on Amazon are HERE. Other clinicians who felt comfortable introducing themselves and why they wanted to come to the group also shared.
We explained that because “this body” is Deaf, and my cochlear implants can only hear one sound at a time, we are going to use the “raise hand” feature in our zoom discussions, just so that I can hear and see who is talking. It was fun that another therapist showed they can use american sign language!
Broadening Our Understanding of Trauma and Dissociation
We talked about how one of the reasons lived experience is really important is because it helps us broaden our understanding of trauma. Often when we talk about trauma and dissociation, we are assuming or referencing childhood or “developmental” trauma. This is called “Dyadic Trauma”, meaning that it is between parent/caregiver and child. There is also “Intergenerational Trauma”, which is when Dyadic Trauma gets passed down to and/or re-enacated with the next generation. We also talked about historical traumas (slavery, colonization, forced migration, genocides as examples) and collective traumas (specific groups of people, such as the Holocaust, or a school shooting, the pandemic, disability groups, or LGBT*). In the past, we have done trainings where we defined those different kinds of traumas like this:
Dyadic Trauma is about what happened in the past.
Intergenerational Trauma is about what is happening again.
Collective Trauma is about what happened to us together.
Historical trauma is about what is still happening to us because of what already happened to us.
We also spent some time talking about neglect, specifically. I quoted John O’Neil (pioneer in the field of trauma and dissociation, author of the primary text known as “the Brick”, and previous guest on the podcast), who said that “it’s not just the bad that causes harm - it’s the lack of good that allows it”. If there is no neglect, there is also no harm or abuse. Developmental trauma always implies neglect at some level.
That being said, we also talked about how neglect is often invisible, and much harder for clients to tolerate discussion of and processing. This also connects back to attachment, and “mirroring”, too. We will talk about all this more in future discussions. I did reference that a new episode with Steve Gold expands the idea of “neglect” to a broader understanding of “deprivation”. Here is that episode:
Our guest this week is Steven Gold, PhD. We talk about trauma, neglect, and dissociation, and he shares about how he broadens understanding of all these terms. We also talk about attachment and the "mirror" of how we see ourselves.... and what happens when there is no mirror, when the mirror is broken, and when there are lots of mirror attempts. We also discuss re-enactments and increasing our capacity for healing.
In our discussion about dissociation, we explored the two main theories of dissociation, one of multiplicity and one of divisibility.
The traditional view of dissociative disorders has been one of multiplicity (literally, Dissociative Identity Disorder previously being called Multiple Personality Disorder). In this theory, there is the concept of the person having more than one personality. Some theories say this develops because of trauma, and some theories say this develops because of attachment. We will talk about those issues in future discussions. But they share a common understanding of “alters” or “parts” or “self states” as distinct personalities.
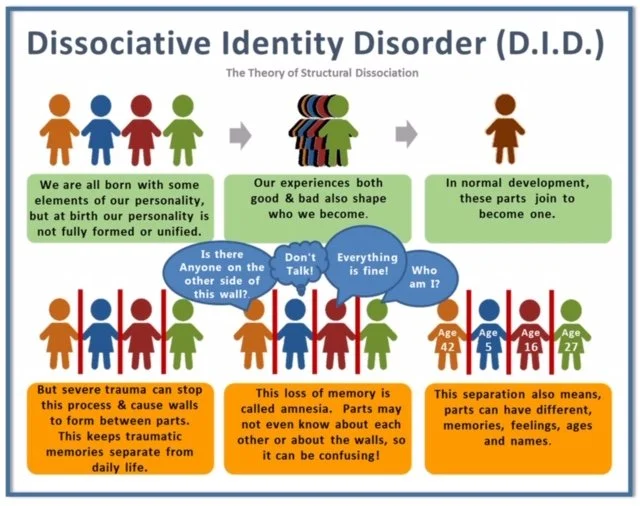
More recently, there has been a movement of “structuralists”. The structural dissociation theory was presented as a concept at a conference, and then popularized via the Coping with Trauma-Related Dissociation: Skills Training for Patients and Therapists workbook. This clarified the idea that all people are born not-integrated, but through healthy development and attuned caregiving, natural integration occurs. Trauma, however, interferes with this process, leaving the person un-integrated. Here is a graphic that shows this, as drawn by someone with lived experience (which I share with permission in our workbook, and which you may share as long as you reference System Speak per artist request):
We also talked, then, briefly, about how OSDD and DID are really mostly treated the same. Diagnosis can be irrelevant outside of insurance or other documentation requests, unless it is just important to the client. At the very most basic level, the only difference in diagnosis has to do with where the amnesia is showing up (or not), which we will talk about in future discussions.
So, in comparing the multiplicity model and the structuralist (divisibility) model, the primary difference is that the traditional multiplicity model (which I prefer) considers each “part” (of the person) to be a distinct personality, while the structuralists consider each “part” to be a part of one overall personality.
[I talk more in depth about this in a CE presentation I do - next time I do that one online is all day April 21st if you want to save the date - 6 CEs!]
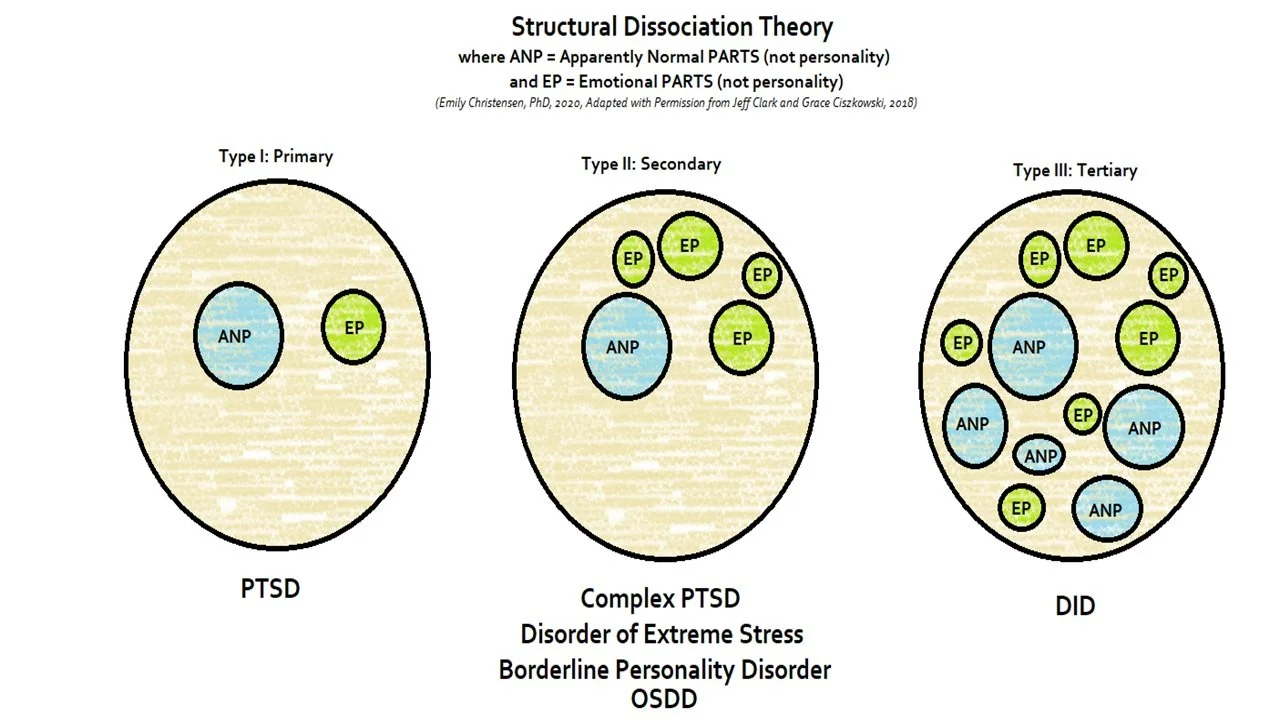
To explain this, we talked about ANP’s and EP’s.
ANP means “Apparently Normal Personality”, and refers to the self-states that do daily life functioning, like going to work or school, parenting, or whatever that kind of functioning looks like in someone’s life.
EP means “Emotional Personality” and refers to the self-states that hold big feelings, trauma, or specific memories.
Part of what structuralists did, then, was to change the “P” from “personality” to “parts”. For structuralists, ANP means “apparently normal part” and EP means “emotional part”. Do you see the difference?
As a Deaf person, I am very visual so drawing things out sometimes help. I made the following graphics to help show the difference the two theories. You are welcome to use them and share them (crediting System Speak) if you find them helpful.
The traditional multiplicity model would look like this, with OSDD and DID having multiple personalities, any of which could experience ANPs or EPs:

In contrast, here is what the structuralist model looks like, where any ANPs or Eps are parts of ONE personality:
From a lived experience perspective, structuralists get many things right..... structural dissociation normalizes that everyone experiences "parts", that integration is part of normal and healthy development in the context of good/safe/attached caregivers, and that trauma interrupts this process. Those are really helpful things.
But, that distinction in parts or personality is really kind of a big deal in experience. It also becomes problematic when clinicians don’t realize what they are saying or talking about, leading to incongruence between what the clinician is trying to offer and the client is actually receiving or experiencing. This is why I do not like “parts” language, even though it is the easiest to say.
The other piece that lived experience often does not like about the structuralists is that traditionally many of them have said NOT to talk to parts or littles or anyone other than the adult part - specifically, that you have to do an adult part who can do therapy. While many with lived experience bristle at this because it feels dismissive, structuralist clinicians are not TRYING to be dismissive - remember that they are considering only ONE personality that has parts, so they are saying this about talking to an adult part because they already have a framework of one personality in parts, rather than different parts. But from a lived experience perspective, it feels dismissive, restricts internal access to therapy, and hijacks which part has control. We can talk more about this in future discussions, but please, in your session, work with what (or who) is presenting.
The other main piece is the "Coping Skills" workbook the structuralists put out is all great stuff for one adult personality who has access to their left brain and frontal cortex, and enough experience in therapy to make those skills procedural memory. But in other situations, the help that workbook offers is limited because healing happens relationally and experientially, which is tricksy to do in a manual. We talked about how a person cannot “think” their way out of trauma.
I do appreciate how many structuralists have listened to lived experiences somewhat in recent years, and adapted and grown and strengthened their positions in that way... for example, in 2021 Kathy Steele reported she has gone from ANP/EP language back to "ego states", which I think is excellent, and van der Hart made the following changes: "levels" of dissociation to "degrees" of dissociation, acknowledging a broader understanding of disassociation, emphasizing multiplicity in divisions of actions (as unique to DID), and stating now that "ego states" is not even strong enough a term to describe multiplicity... the exact quote from his paper is: "dissociative parts of the personality may comprise any number of psychobiological states, which implies that labeling them as ego states or self-states is giving to them too low a degree of reality". (van der Hart, O. (2021). Trauma-related dissociation: An analysis of two conflicting models. European Journal of Trauma & Dissociation, 5(4).)
I talk about all this more in my trainings.
Discussion with Clients
We shared some about how different clinicians share about dissociation with their clients. We talked about the importance of going slowly, about the client being able to tolerate awareness even before being able to explore, and we talked about different ways to discuss it with them as they are ready.
One clinician shared that they emphasize the gift and capacities of the mind to protect and help through difficult situations.
One clinician shared about normalizing dissociation by using the idea of a continuum, like how all of us experience highway hypnosis where you miss your exit, to DID being the other end of that spectrum.
We also shared about sometimes explaining the science of what is happening in the brain (i.e. polyvagal theory) to normalize or to keep ANP or cognitive focus online while talking about it. If you want to know more about polyvagal theory or the science of dissociation, we recommend this episode:
Dr. E interviews Dr. Dan Siegel of the Mindsight Institute, who defines dissociation by defining integration by defining differentiation. He explains interpersonal neurobiology, and how that has everything to do with DID but is also bigger than that. He then defines developmental trauma as an assault on integration. He then explains the science of why and how this is, and what hope it gives for healing.
This lived experience episode really goes with the Dan Siegel one:
We share the processing we have done following the Mother Hunger episode and the interview with Dr. Siegel. We share how understanding what Dissociation is actually helps us deal with both false beliefs from shame and the protective denial that comes with it. We explain how Dissociation isn’t just avoidance of what was bad, but avoidance of the realization we couldn’t do anything about it. This tells us, we learned, what the wall of terror is and how to get through it.
Here is the “Mother Hunger” episode referenced in Wall of Terror. These three episodes together really are a great example of working with the left brain, the right brain, and the integrative processing of those two experiences coming together for breakthroughs in healing. This episode is also an example of addressing some of those neglect or deprivation issues we talked about earlier.
We speak with Kelly McDaniel, who coined the term Mother Hunger. She explains what this means, and how it is the earliest trauma and a disenfranchised grief. We discuss not having “permission” to talk about our mothers, much less work out mother trauma, which leaves us isolated from mothering and healing. In this, she is able to explain how and why dissociation starts in infancy - and what it is protecting us from exactly. Trigger warning for mother related content, and reference to the mother-baby dynamic, though no specific abuse stories are discussed.
Finally, another clinician recommended this episode as an example of the neuroscience and how the brain works, for those who are trying to learn more about that to understand (and validate the legitimacy of) dissociation or to be able to better explain it to clients:
We welcome back Christine Forner, to share after the virtual ISSTD conference. She talks about the “Cascade of Defense”. She explains Active and Inactive Defenses. She gives feminist context to survivor experiences and treatment.
Another clinician shared about how they present the idea to clients that the “host” or ANP or presenting part in session is ALSO a part, not just that they are one who has parts. We will talk more about this later.
Tools for Treatment
We talked about CBT and DBT being more of those good “skills” many survivors need, but again how those skills are only accessible when the frontal cortex is online. We also talked about being wary of “trauma-informed” models that are not actually, because dissociation and long-term diagnoses are ruled out of participating in “evidence-based” therapies. Susan Pease Banitt talks about this in her book if you want to read more. Her episode is here:
Dr. E interviews special guest Susan Pease Banitt, LCSW, author of “The Trauma Toolkit” (for survivors) and “Wisdom, Attachment, and Love in Trauma Therapy” (for clinicians). In a poignant moment before the interview even begins, Dr. E is startled by the compassion offered by her guest. Susan Pease Banitt shares the history of healers, explains about holistic healing, and teaches about acknowledging our own vulnerability. Due to the nature and content of the interview, some triggering topics are referenced, such as types of abuse including ritual abuse. However, no detailed stories or examples are given in this episode.
We talked about how IFS, or Internal Family Systems, uses “parts language”, but was never meant to be a model of therapy for trauma. It has since been adapted by many, like Janina Fischer, who have excellent books or tools and flip charts and all kinds of resources to use with trauma and dissociation. We are about to interview Joanne Twombly on the podcast about her new book adapting IFS in helpful ways. These are all great things, and I do not mean they are bad clinicians. They help so many, and it's good stuff!
But when people only get a basic training, or only use tools as methods, and don't have the background or experience to also include relational or psychodynamic. etc., it very quickly becomes problematic as improperly manualizing a method that was never meant for what they are trying to help heal.
IFS (generally) also has several things two know that clinicians new to trauma and dissociation sometimes forget:
1.) that it is very structural dissociation, which is great in some ways, but has challenges and limitations as already described - increasingly so as it gets passed down poorly to clinicians with less education or experience.... especially as it assumes some psychodynamic training that no longer happens in graduate school like it used to;
2.) it is anti-polyvagal theory, in that it considers any dysregulation as another "part" even if it is in the body (nothing to do with personality at all); and
3.) this means also that it does not believe in a phase-based approach, because there is no need (according to them) for safety and stabilization when the dysregulation is part of what they are talking to (so don't want to get rid of, but work with).
That being said, there is lots of good material if you can keep those ideas in context, and do the work to balance it out and keep your clients safe. Here is an episode we did recapping a Janina Fischer webinar, where we talk about being wary and then discovering so much good in what she taught:
We welcome back (new) Julie to recap with us the ISSTD Webinar featuring Janina Fisher. We discuss alienation of self, underlying needs of trauma responses, and healing through compassion.
We also talked about EMDR being an effective tool for treating trauma, but not being a complete method to address deprivation and capacity building. These aspects of trauma and dissociation need psychodynamic and relational therapy, utilizing the actual relationship with the therapist for experiential healing. EMDR can still be very useful and effective for very specific traumas, but needs a broader foundation to utilize safely with dissociative clients. We also need to be aware of how much EMDR took from hypnosis, which is not discussed enough, but we will keep talking about in our discussions! For EMDR training appropriate for dissociative clients, I would recommend Jamie Marich with her Insittute for Creative Mindfulness (lived experience) or Michael Coy with ISST-D (more academic, good foundation of hypnotic training, dissociative-sensitive). Both presenters are LGBT* safe.
Another clinician also shared about the importance of and role of induction, which we can circle back to more later, as well, when we talk more about trance logic.
CHALLENGE
We challenged group members to choose one of the clinical interviews from the podcast (you can see a list HERE) to listen to before our next month’s discussion, and come ready to share something that was new to you, different from your own perspective, or new material that you learned.
Someone requested we talk more about assessments, and I shared THIS LINK for free public access to some screening tools. We can pick up there next month!
Our next “First Wednesdays” discussion group will meet April 5th, 2023!
CLICK HERE to return to the Discussion Group Monthly Recap page.